What is Ageing?

Physiological changes in the body are a natural part of aging

Physiological changes occur in almost every organ system in the body

Genetics affect aging

Many diseases and conditions become more common

Psychological and social issues play a role in physical and mental health
Normal Aging
“Growing old is mandatory, but growing up is optional!” – Walt Disney
“Ageing is just another word for living.” – Cindy Joseph
“Getting old is like climbing a mountain; you get a little out of breath, but the view is much better!” – Ingrid Bergman
“The best tunes are played on the oldest fiddles!” – Ralph Waldo Emerson
Age Related changes in Muscles and joints
– the aging process
“The impact of a normal aging process on skeletal muscles and joints can have profound effect on the functionality of an individual ” – Mohamed S et al.
Programmed theory – follows a genetic timetable.
Damage theory – cumulative consequence of free radical reactions. Source of this toxic substance can be in environment or byproduct of cellular metabolism.
Normal aging does cause loss of motor units and the number of muscle fibre bundles that one nerve feeds into.
The age related loss in active motor units means 25% motor units become non functional from age 20 to 80.
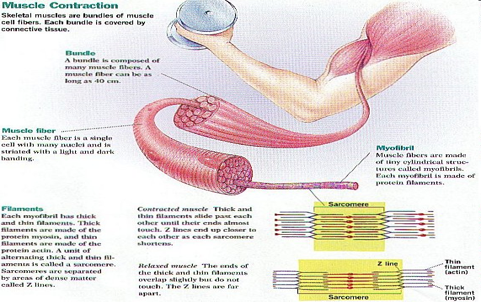
Slow twitch fibres– long acting type 1- aerobic only. For endurance activity – more mitochondria, myoglobin and capillaries /square inch of muscle.
Fast twitch fibres – short acting type 11- can derive energy for periods of time, from anaerobic metablism- strength and power in movement.
The reality as we know it- normal aging process
As we age, skeletal muscle changes are related to inactivity, underlying medical conditions, poor nutrition, cellular changes and hormone changes.
Age related changes vary among muscle groups and muscle fibre types and do not affect all muscles equally.
- Muscle mass decreases with aging affecting total body weight
- Young healthy person 30 % is muscle mass and 20 % adipose tissue and 10% bone.
- By age 75 about 15 % is muscle mass, 40% adipose tissue.
- Strength declines 1 to 2 %/year between 65 and 89 years of age.
- Power declines by 3.5% annually between 65 and 89 years of age.
Normal aging and muscle function
Upper limb strength in normals decreases with age after the age of 40 at a rate of 1.5% per year. Beyond the age of 60 and in 70s it decreases at 3% per year.


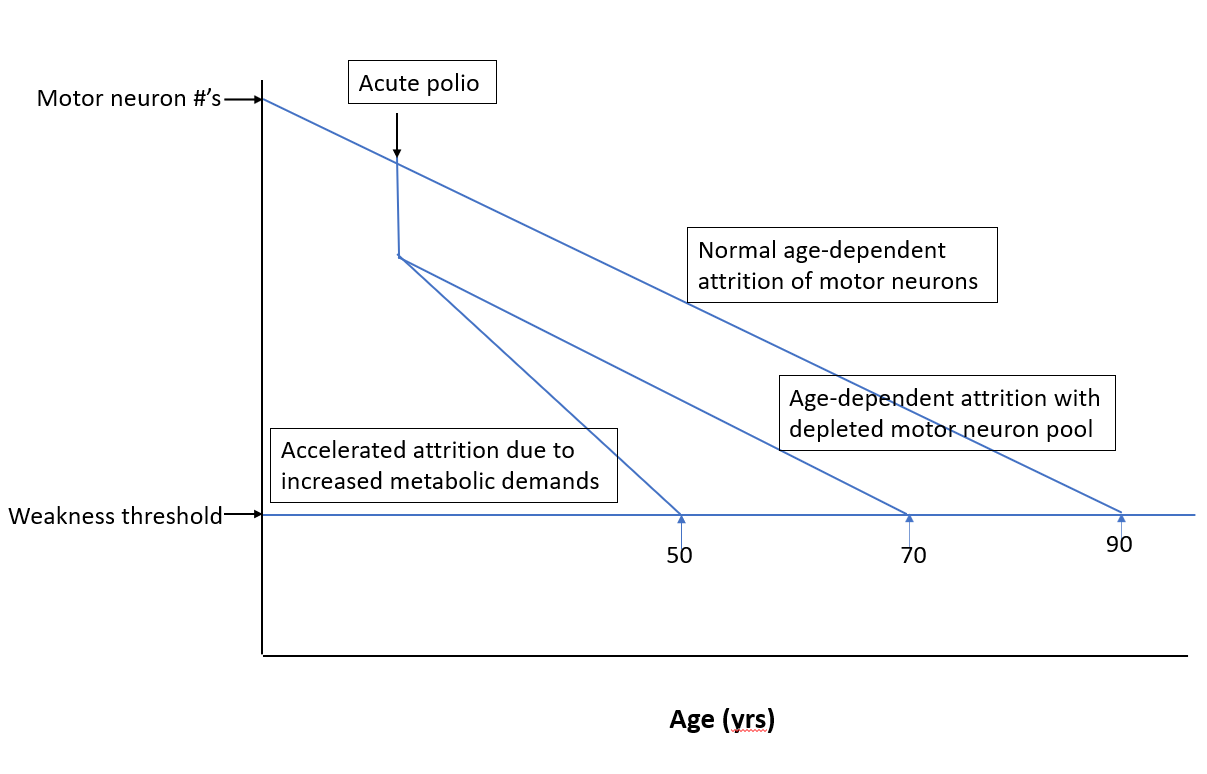
Age related changes in polio
- For those who have had Polio the rate of decrease is at 11.2% per year beyond 40 years and 17.5% in 60s and 70s.
- Lower limb strength in polio is not age related, but related to the amount of initial damage.
- Aging muscle with the reduction in size and total number of strength and power muscles and reduction in number of endurance muscles.
- By 70s and 80s maximal voluntary contractile strength is decreased by 20-40%.
- Muscle mass is the determinant between age and gender related difference.
- This relates to your ability to lift a load –lift luggage, lift shopping bags, lift a pail of water.
- Max isometric force decreases by 20% in 60s and by about 50% in the 80s.
This affects your ability to sustain a load e.g:
- Carrying a pail of water from tap to the garden .
- Carry the shopping from the car to the kitchen
- Carry your luggage to the car.
Pathophysiology involved in aging muscles.
Motor unit re-modelling is a process whereby there is selective denervation of muscle fibers and re-innervation by axonal sprouting from adjacent motor units.
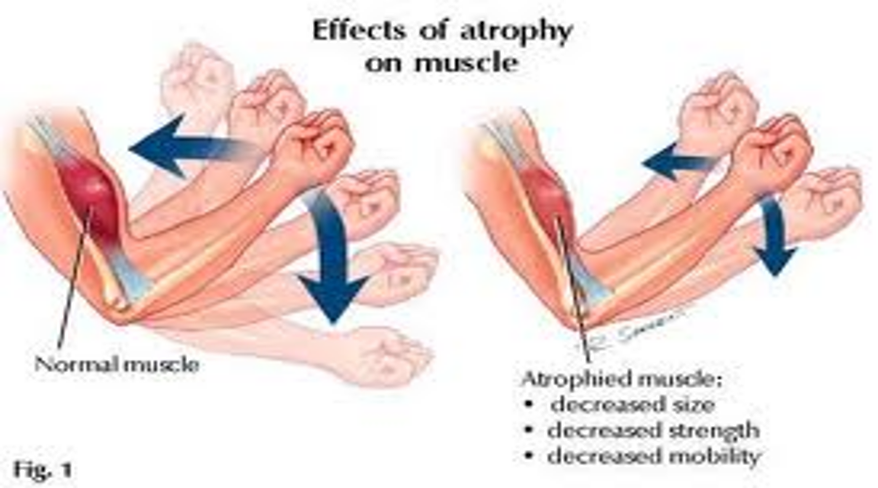
Consequently there is a higher portion of denervated muscles and muscle atrophy.
Changes that take place in a muscle cell as it ages.
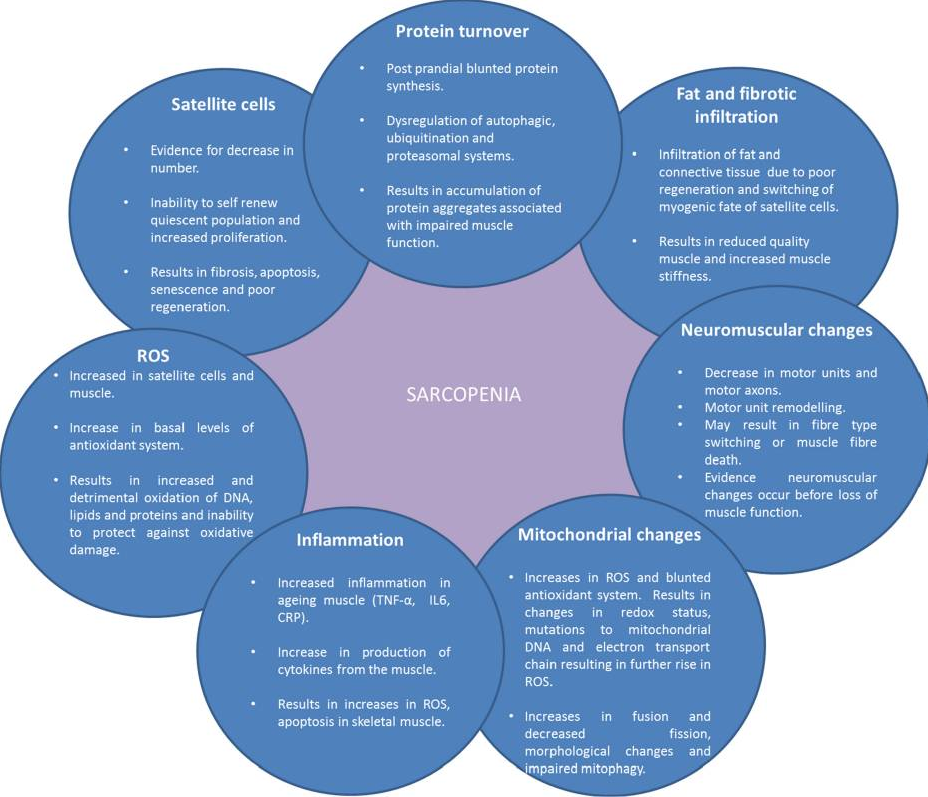
Loss of satellite cells with aging – cells that support new muscle tissue and repair = reduced ability of muscles to regenerate after injury or overload.
Reduced oxidative capacity in mitochondria, up to 50% /volume of muscle in older adults – leading to reduced ATP production – reduced ability to produce energy = muscle fatigue.
Decreased rate of protein synthesis – due to reduced synthesis of protein from amino acids, leading to loss of muscle mass.
Reduced motor unit firing – associated with increased presence of fibrotic tissue, impaired healing of injured muscles and increased fatigability.
A consequence of micro-tearing of muscle over time.
Every fall, every sprain and every strain causes micro tearing of muscle fibres and ligaments.
Absolute bed rest can accelerate loss of muscle mass and strength at rate of loss of 1.5% /day- affecting anti-gravity muscles most. These are the muscles that maintain posture in standing.
Pain inhibition, e.g. back pain, leads to atrophy or loss of muscles that help to maintain standing. Moving is easier than standing
Four reasons principles for aging people who had polio
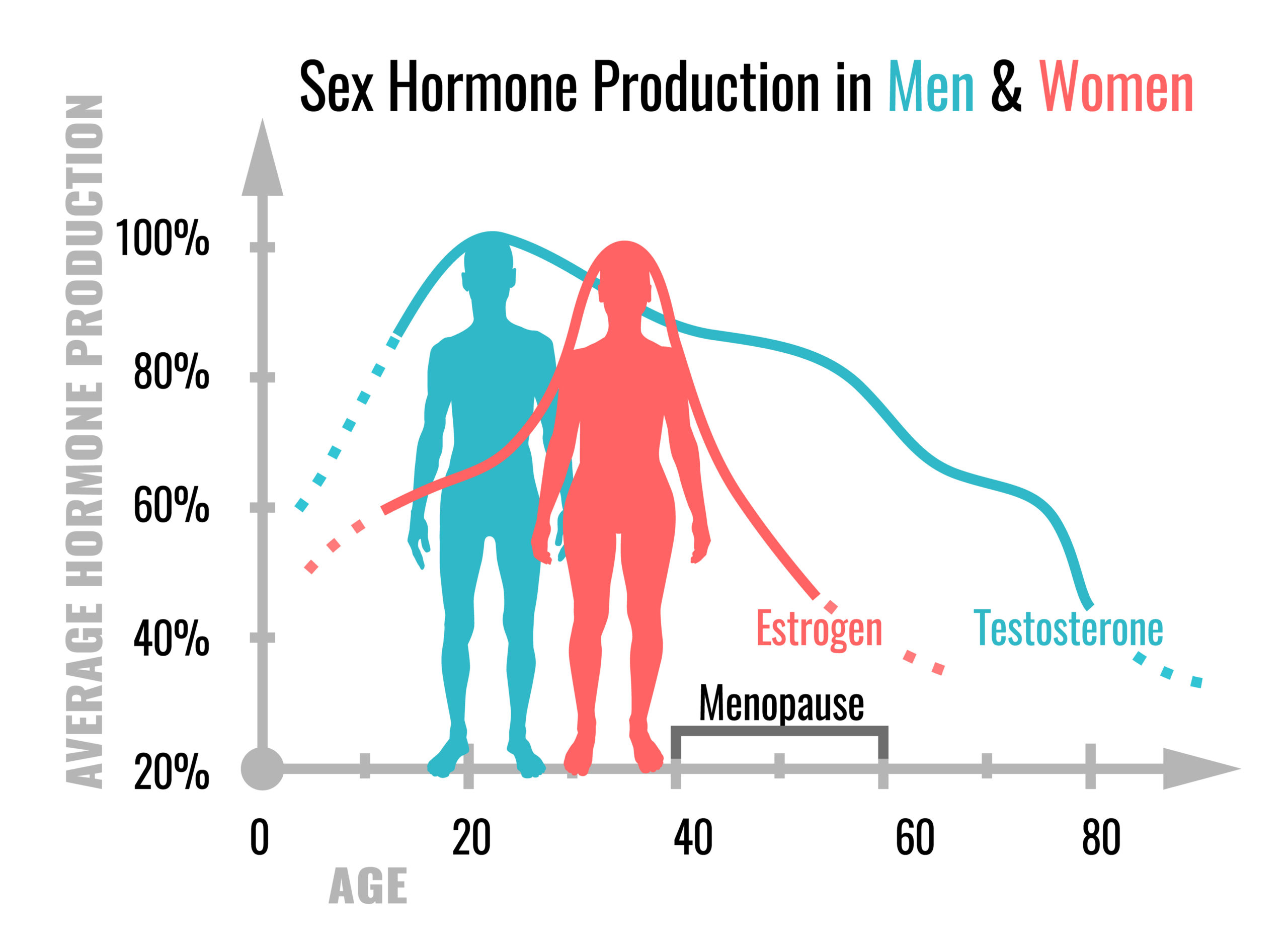
Hormone changes part of the aging process
Men – Decreased testosterone in men has been associated with decrease in whole body protein anabolism , decreased strength, decreased fat oxidation, and increased adiposity.
Women – 15% decline in muscle strength around menopause- decrease in estrogen.
All above impact on normal muscle function, leading to impaired gait and balance, leading to higher risk of falls. This in turn impacts of functional mobility/capacity.
Aging effects on organs : Cardio-pulmonary changes.
As you age organs loose some function
Structural changes in bones, cartilage and elastic structures
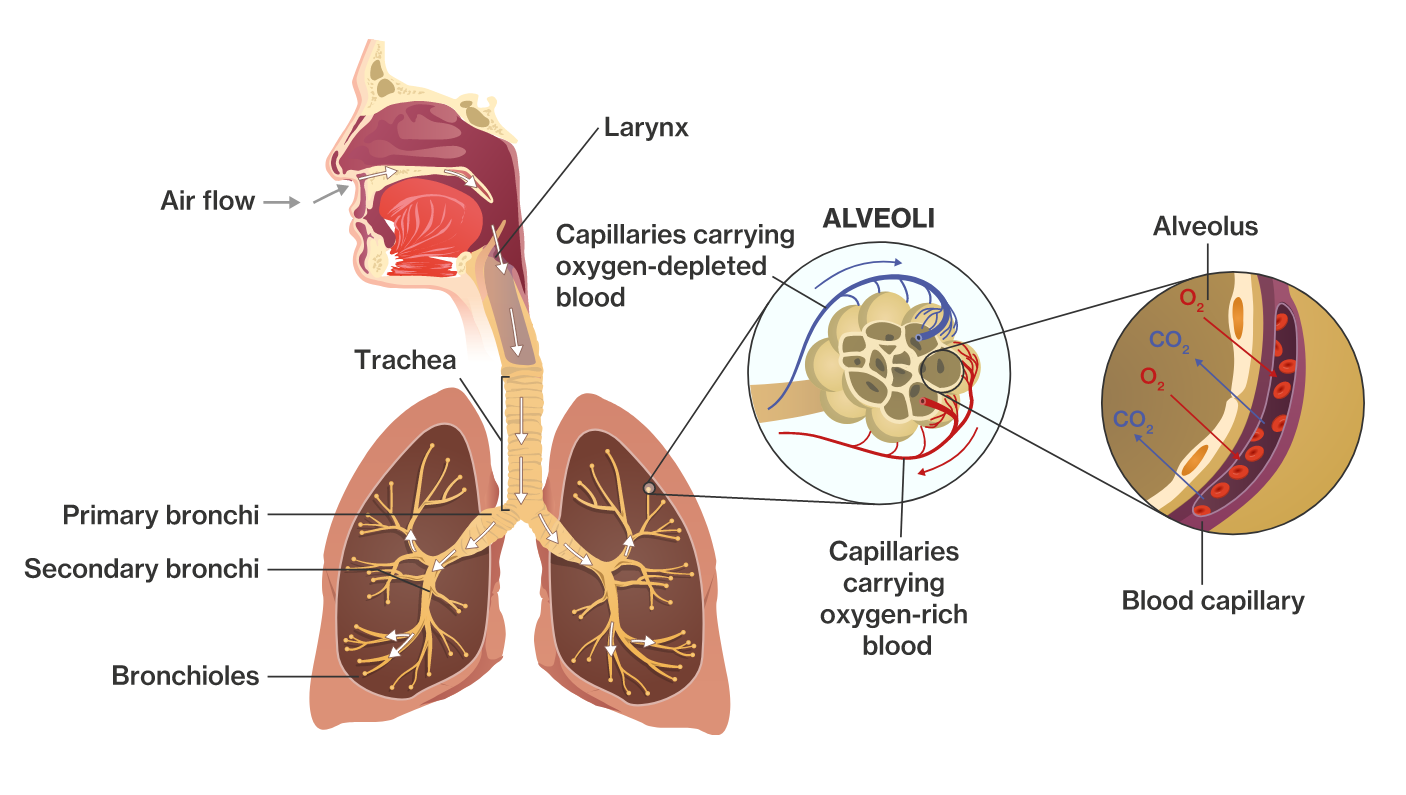
- Lungs become less elastic – age 25 to 65
- Vital capacity decreases by approx. 20%
- Forced expiratory volume decreases by approx. 10%
- Residual volume increases by approx. 10%
- Increase in dead space leading to decrease oxygenation in blood.
Increased work of breathing
- Loss of alvelor tissue and septa
- Decreased total surface volume for gas exchange
- Changes in smooth muscle structure
- Increased thickness of musocal bed.
- Increased rigidity of tubular structures.
Structural changes in elastic tissue and muscle of the Heart
- Changes in cardiac valves, reduced elasticity
- Reduced distribution of blood flow in the lung and to all the muscles in the body.
- Changes secondary to co-morbidities:
- CAD- coronary artery disease/ IHD- ischaemic heart disease.
- Chronic lung diseases.
- All lead to loss of energy and reduced muscle bulk.
Aging effects on organ systems e.g. Balance and Movement
- Visual, somato-sensory and vestibular systems-feed forward loop: With a decrease in information about orientation and movement of the body in space
- Central processing: Increase in response time- slow processing of above information by the brain
- Motor system – effector pathway/feed back loop. Delayed or poor motor response, poor coordination, loss of balance/fall.
Common symptoms of ageing include:
Skin and hair becomes thinner, more fragile and dry
Muscles become smaller
Joints accumulate wear and tear
Skeletal alignment becomes shorter with increased spine curvature
Decreased sensation in your hands, feet, arms or legs, the gradual loss of your eyes’ ability to focus on nearby objects and hearing loss
Changes in Ageing – Getting older and living with the late effects of polio
In 1987 Halstead described created the condition called Post Polio Syndrome. Living with the Late Effects of Polio is what many call the experience of growing older having had polio as a young person. They both involve getting older (hopefully)! This can be a double whammy – as they say “Old age isn’t for the faint hearted”. If that is the case then, “Old age and polio isn’t for the even moderately brave” and because of that, not easily understandable by the mainstream. Equally underappreciated can be the skills and attributes we have had to develop to survive and thrive.
I
Four reasons why people who had polio may be really good at aging .
What can I do to improve my Ageing?
Here are some key principles:
Embrace lifestyle changes including pacing activities, eliminating bad habits, reducing stress, optimising a good diet, getting adequate sleep and asking for help when needed
Identify risks – use safety and fall prevention measures – develop an individualised exercise program
Get regular medical care/ screening, optimizing health management of medical conditions. Get vaccines for flu, pneumonia and Covid-19
Find enough joy in the day to balance the challenges we face every day
Social Effects of Ageing
Ageism and ableism combine for every disabled person as we grow old, a double filter in our connection with the world. It is not personal in that the cultural stereotypes are embedded in all and act as general templates for how we relate.
It is personal in that our sense of belonging and access to resources depend on how we feel we are being treated. Our sense of wellbeing is tied to our sense of belonging, be it to relationships, a community and place through whakapapa and history.
Just as our bodies are changing naturally through aging, so is our sense of well being, self understanding and ability to utilise our dis/abilities.
Find out more
Resources, Links and Research Downloads
Perceived consequences of ageing with late effects of polio and strategies for managing daily life: a qualitative study.
Q: The aim of this qualitative study was to explore how ageing people with LEoP perceive their situation and what strategies they use for managing daily life.
W: Seven women and seven men (mean age 70 years) were interviewed.
A: Ageing with LEoP affected daily life to a great extent emphasising the need to design rehabilitation interventions that focus on coping, empowerment and self-management for people ageing with LEoP.
